Perpetual dependency is debilitating and breeds only resentment and envy.
Ray Krause, O’Neals
This article examines charitable giving and the use of donor funds in the charitable healthcare sector, aid primarily earmarked for disadvantaged communities across the globe. While it is true that much of this money has reached it’s target audience, it is the manner in which it is utilized in these communities and the dependencies it creates that are of grave concern.
In the last decade we have disbursed over 500 billion dollars to health related care, much of it on the African continent. In the next decade we will spend even more, if our global economy is able to support it. Why? Why, after decades of pouring eye-watering sums of money into what appears to be a bottomless pit, are we no closer to the espoused goal of Universal Health Care or at the least, more robust and independent health systems in the communities we assist?
The answer is a simple, yet unpleasant one. Out of choice. We choose to perpetuate these dependencies and where possible, create new ones. A profit driven Western health system dictates it and charities comply, whether out of complicity or a desire to serve these vulnerable populations in any way possible, even if the mechanisms are flawed. Charity is big business. Consider this 500 billion was spent on healthcare alone.
To understand how we’ve arrived here and why the historical actions of charitable health outreach have created global dependencies requires background knowledge of the healthcare sectors, the non-profit industry, and the mechanisms that enable and support global health outreach. Central to this is acknowledging the ever expanding elephant in the room.
Our inability to step away from the flawed systems that power healthcare and how these systems and policies impact our ability to deliver meaningful aid lies at the heart of the problem.
While this article uses the terms charity and non-profit organization they should not be considered as inclusive of the entire charitable industry. The terms are used here in the context of those organizations that provide health related care, services and support globally.
Separating health based donations from general charitable donations isn’t a simple ask, as many charities engage in activities that cover more than one aspect of aid delivery, catering to both health and humanitarian services. There are a few figures below to allow you to form a clearer picture of the numbers involved, keep in mind however, these are not all health related.
A landmark study in 2018 identified 250,000 foundations across 38 different countries. 72 percent of these were established within the past 25 years. The highest concentration of foundations is in Europe (154,271) while North America also has a considerable number (91,850). Unsurprisingly, they tend to be more common in high-income countries where they control serious levels of cash.
The following infographic shows the assets held by philanthropy foundations at country level. The United States leads the way with $890 billion while the Netherlands comes second with $108 billion and Germany is third with $93 billion. China is also present on the list, rounding off the top-10 with just over $14 billion.
How is this money allocated? Another survey by BNP Parabas released in 2015 and published in Forbes in the same year, offers some insight. Refer to the infographic below. American individuals and companies donate hundreds of billions of dollars to charity every year. In 2016, donations reached an estimated $390 billion, according to a report by Giving USA.
As is the case in most years in the US, religion was the sector that received the most money in 2016. It accounted for $122.94 billion or 32 percent of total philanthropic giving in the U.S. in 2016 Education came second with $59.77 billion while human services rounded off the top three with $46.8 billion. Where did this money originate? The public were in first spot, accounting for 72 percent of the $390 billion total – $281.86 billion. Foundations gave $59.28 billion and corporations donated $18.55 billion in 2016.
The chart below, courtesy of Giving USA, represents a breakdown of these figures for 2022. Note the growth from $390 billion in 2015. Beside the chart is a graph, reflecting the corollary effect of a strong stock market on giving, a link that currently threatens charitable giving for the first time in over a decade.
Donor government funding, including both the bilateral funding given directly to other countries (which may be given to a country government or provided to NGOs and other organizations to carry out work in recipient countries) and the multilateral funding given indirectly through contributions to multilateral organizations, accounts for most external health aid channeled to the developing world. As such, this donor support constitutes a major component of the global health response.
Donor government funding for global health has risen significantly since 2002, growing from $4.4 billion to a peak of $22.8 billion in 2013 (see Figure 2). However, funding declined for the first time in 2014 to $21.5 billion and has since remained relatively flat.
Donor government funding for health has generally increased as a share of official development assistance (ODA), particularly over the last decade. These increases were largely spurred on by the creation of several new funding initiatives and mechanisms such as the Global Fund and PEPFAR. However, this share has remained essentially flat in more recent years and declined in 2014 and 2015. This flattening and recent decline has raised concerns about the ability of countries to meet global health goals and targets, such as those of the Sustainable Development Goals (SDGs).
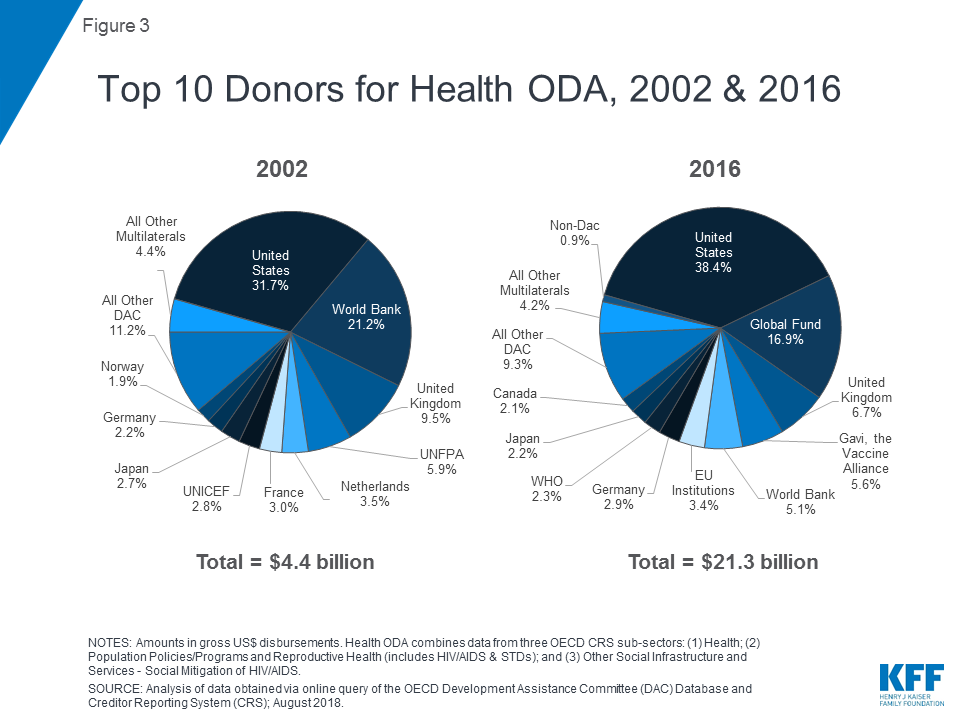
The U.S. has been the largest donor to health in each year over the entire period between 2002 and 2016, and has dedicated the greatest share of its ODA to health. The donor mix has shifted over this time, in part due to the entrance of new donors, particularly the Global Fund, which became the second largest donor to health after the U.S. in 2006 (and remains so today). The U.S. and the Global Fund combined accounted for more than half of total donor funding for health in 2016 (see Figure 3).
While figures are easy to find for individual countries, finding global ODA spends are more complex. To really quantify the efficacy of health based charitable activity, we need to understand how much money has been thrown at global health over the last decade and why we are still faced with increasing demands for ever more aid, despite the donations spent. The graph below shows a breakdown of ODA Health allocation by country for 2021.
Adding together figures for the last decade1 (2012-2022), we arrive at the eye watering amount of $245 billion dollars, ODA funding, designated directly for charitable healthcare. This does not include billions more, raised directly from the public and foundations, earmarked for the purposes of improving health outcomes for disadvantaged communities across the globe. A more realistic figure that would include these donor populations would be in the region of $500 billion dollars.
Lets put that figure into context. It is the equivalent net worth of Bernard Arnault, Elon Musk and Jeff Bezos, the three wealthiest individuals on the planet, combined. If it were a country, it would rank 25th based on GDP, somewhere between Poland and Belgium. Yet, for some inexplicable reason, in 2023 we will require more funding than ever to address global health disparities, and in 2024, we will require even more money.
Almost all large charitable organizations tasked with the delivery of health to developing countries intentionally create delivery mechanisms that encourage dependency on continued donor aid.
This is fact, If the focus of their work had been enabling downtrodden countries to develop self-sustaining methods for delivery of care that included strengthening health systems in-country, $500 billion dollars would have been sufficient to put most of these charities out of business by now, which, in an ideal world, would be seen as a stunning success. The reality however, stands in stark contrast.
To FIAT driven enterprises, captive audiences matter. Few industries, if any, are able to eclipse the potential for profit shown by healthcare. Their global market of patients continues to expand, this expansion matched only by a sharp upturn in the maladies afflicting the burgeoning numbers. We are getting sicker, earlier, and in larger numbers, from an increasing number of conditions, many previously considered rare, now chronic.
Emphasis for care has pivoted over the last few decades from curative to treatment based. We no longer seek to drive back disease, merely manage it. From a business based perspective, managing a sick patient, sometimes for decades, represents the gold standard of “captured market” profitability. Charities play their own, if unintended role in this play for profit, providing a vital funnel to large, otherwise inaccessible markets in developing countries.
In 2019, in the US alone, charitable institutions and non-profits employed over 12 million people2. Their payrolls eclipse other large industries, including finance and construction. Providing for those less fortunate has become big business and as is inevitable with any booming enterprise experiencing growth, problems abound, some of which are inherited or enforced from supporting industries (read healthcare) while others are self inflicted. It is the beneficiaries of these charitable health enterprises that pay the associated costs.
While protracted treatment has become the mainstay of modern healthcare in developed nations, in developing countries the emphasis is placed on creating dependency. Charities that encourage and promote funding dependent projects and outreach. Missions that are cyclic by nature, repetitive and that require a continuous influx of donor capital to deliver care. This creates the necessary cycle essential to cornering a captive market.
Dependency is the goal, rather than an unintended consequence.
While the argument exists that the delivery of care and saving lives trumps the flawed methods of delivery, the current system suffers from various weaknesses, weaknesses that expose communities that are forced into aid-reliant dependency to risk, often life threatening in nature. Weaknesses that, under the right conditions, could collapse global health efforts and the elusive goal of universal health care.
Why not then develop care delivery systems that encourage self-reliance and that are self-sustaining, that integrate with and strengthen local healthcare systems, and remove these dependencies? If you’ve been paying attention, much of what you’ve just read goes to the heart of the matter. Captive markets matter and no where was this more clearly illustrated than during the Covid pandemic of 2020 that shut down the entire globe.
These dependencies are furthered by funding directives for foreign aid. As an example, EU countries under duress to meet targets issued by organizations like the WHO, pay over billions of dollars each year. To avoid missing quotas and to minimize workloads, large scale donations are the norm. Amounts often in excess of a $100 million dollar are granted annually, to single charities. This encourages poor business practice and suspect oversight, where auditing and controlling donated funds at scale becomes an impossibility.
AT the other end of the table, the benefiting charities are faced with the need to dispose of these huge sums within a calendar year or run the risk of missing the following year’s handouts. The system is antiquated, littered with loopholes for financial exploitation (which occurs all to frequently) and clearly not fit for purpose. It is revolving door, disposing of capital to keep up with quotas at a dizzying rate, one that does not allow for circumspection, investigation and oversight.
It is fertile ground for exploitation for the sake of profits, by an industry (healthcare) that has shown itself all to capable.
Whole industries have grown up in and around the delivery of charitable health care, providing product to the captive markets who have come to depend on Western charity, often with their lives. Most who operate within this system recognize it for what it is, but will not rock the boat. The stakes are too high, the profits too enticing.
So how are the billions spent and where do they originate?
The best known target in international aid proposes to raise official development assistance (ODA) to 0.7% of donors countries national income. In 1970, The 0.7% ODA/GNI target was first agreed and has been repeatedly re-endorsed at the highest level at international aid and development conferences:
The OECD Development Assistance Committee (DAC) is a unique international forum of many of the largest providers of aid, including 31 member countries. In 1969, the Pearson Commission proposed a target of 0.7% of donor GNP to be reached “by 1975 and in no case later than 1980.” This suggestion was taken up in a UN resolution on 24 October 1970. The target was built on the DAC’s 1969 definition of ODA.
DAC members generally accepted the 0.7% target for ODA, at least as a long-term objective, with some notable exceptions: Switzerland – not a member of the United Nations until 2002 – did not adopt the target, and the United States stated that it did not subscribe to specific targets or timetables, although it supported the more general aims of the Resolution.
In 1993, gross national product was replaced by gross national income (GNI), an equivalent concept. DAC members’ performance against the 0.7% target is therefore now shown in terms of ODA/GNI ratios.
In 2022, official development assistance (ODA) by member countries of the Development Assistance
Committee (DAC) amounted to USD 204.0 billion. The United States continued to be the largest DAC member provider of ODA (USD 55.3 billion), comprising more than a quarter of total DAC ODA, followed by Germany (USD 35.0 billion), Japan (USD 17.5 billion), France (USD 15.9 billion) and the United Kingdom (USD 15.7 billion).
Problems Abound
The DAC has recently changed ODA reporting rules to include transactions that require no financial sacrifice. This deprives ODA of its meaning as a gauge of aid effort, and vitiates the point of setting the U.N. ODA target. The changes have also rendered ODA incoherent as a statistical measure, making it a faulty tool for monitoring and analysis. ODA now fails to meet basic statistical quality standards.
According to a report issued in 2019 by the Brookings Institute3;
ODA was never perfect, and for years critics complained about the inclusion of items—such as the costs of students and refugees in
donor countries—which transferred no resources to developing countries. But since 2014, DAC decisions mean that ODA is not just counting debatable items, but inventing numbers that do not exist in the real world.
Brookings Institute
The report continues to catalogue a list of flawed reporting mechanisms that reduce any meaningful data to spreadsheets of incomprehensible nonsense, with double reporting and other statistical anomalies. The bottom line? Reported donor amounts now need to be taken with a large grain of salt. While it appears on the surface that aid continues to flow in ever increasing amounts from ODA, the real world impacts have been seriously curtailed by an actual reduction in physical money flowing to charities.
As economies begin to contract globally, expect this trend to worsen, with governments taking full advantage of the loopholes created by DAC to claw back funds required at home.
The favored vehicle of a new breed of billionaire philanthropists, charitable foundations are a force to be reckoned with in the charity sector, disbursing billions annually to various causes. The goals and beneficiaries of these foundations align with political leanings and a strong case can often be made about the wisdom of self-created health outreach projects embarked on by these foundations.
The Bill and Melinda Gate Foundation is perhaps most controversial, with ill-conceived vaccination drives in countries like Swaziland, where a focus on reducing maternal mortality by treating HIV led to near collapse of the Swazi healthcare eco-system, and shifted mortality risk from the mother to the infants. Tinkering with fragile healthcare systems comes with consequences.
These foundations are also able to expand and interject personal agendas, financial or otherwise, into global healthcare policy by way of massive donations to institutions like the WHO, and again, the Gates Foundation features prominently. In 2018-2019, the United States was the largest donor to the WHO at $893 million, accounting for around 15 per cent of WHO’s budget. The Gates Foundation came only second, with $531 million, a position the Foundation has maintained for a while.
Critics argue, and rightly so, that foundations like the Gates Foundation hold undue sway over global health policy because of their donations, not only to the WHO, but in the fields of development, policy and advocacy and U.S. education. In 2022 Gates added $20 billion ($5 billion for 2022 and $15 billion for past pledges) to the Gates Foundation coffers, making him the single largest global charitable donor for the year.
Some $8 billion in donations went to foundations in 2022, with $5 billion injected into the Bill & Melinda Gates Foundation alone. The benefit of these donations to the various industries they cater to will not be experienced immediately but rather over many years. U.S. foundations are required to spend only 5% of their assets annually, and most foundations try to preserve their holdings so that they may continue operating well into the future.
Charitable giving in 2022 declined from the highs of 2020/21 to pre-pandemic levels. This decline in giving likely had something to do with 2022’s stock market volatility – major indices lost as much as 33% of their value – and the onset of high inflation. Both financial markets and inflation can influence charitable giving.
How much of this giving translates into actual patient care and how much of it utilized to pursue influence is unclear. What is however abundantly clear, is that both health policy and agenda are for sale for the right price, exposing the global population to healthcare that is decided by a handful of unelected individuals. The dangers of this are self-evident.
In the United States in 2021, the largest source of charitable giving came from individuals, who gave $326.87 billion, representing 67% of total giving. There are numerous factors that threaten this figure’s growth. As global economies contract post Covid and trillions in aid is directed to fund the war effort in the Ukraine funding available for health related outreach will no doubt suffer. We are becoming poorer and one of the first things to feel the impact of this will be charitable giving.
The influence of social media and main stream media also influence giving, earthquake relief in Turkey and other breaking human tragedies are brought (rightly so) to the forefront, jumping the queue and effectively drawing away funding from traditional donations. Increasingly volatile weather patterns, political instability in Europe and other factors will also play a role.
While we may see increases in public giving in the coming decade, traditional charities are less and less likely to benefit as the limited pool of funding is placed under ever increasing pressure to address a multitude of new demands.
Donor apathy also affects giving patterns. We are exposed to visual extremes on a daily basis, numbing us to images of poverty, suffering and need and the constant deluge makes it increasingly difficult for charities to find a foothold for their cause. Without resorting to “poverty porn” to stress the need for funding, most emergent charities find it more and more challenging to raise funds from the public sector.
To effectively address solutions to a problem, either mechanical or system driven, you require two essential components. The first is innovation and the second, is understanding. Why understanding? Simply answered, you cannot create lasting solutions if you do not possess an intimate understanding of current solutions, their histories and iterative evolution.
How we have arrived here dictates how we plan for the future.
The term “improvement” is frequently interjected into discussions. It is a subjective and misleading term. Do we seek to simply modify an existing solution to “improve” outcomes, ensure a tool or system is optimal, or build an entirely new tool? Improvement suggests utilizing an existing solution, system or tool to solve an historical problem by iterative adjustment. To innovators, the term is anathema.
Healthcare, and its delivery is analogous to the above. For the last two decades, iterative jumps in technology have seen existing delivery and supply mechanisms within healthcare “upgraded”, affecting the systemic delivery of care to patients and the ways in which this care is dispensed. Very little of what we have witnessed can be categorized as innovative. “Improvements” abound, and while this process is essential to modifying solutions, at what point do we acknowledge the obvious?
The need to repeatedly “improve” can only suggest one thing. Our healthcare tools, systems and solutions are not fit for purpose. Spillover from the healthcare sector directly impacts the charitable delivery of care. The emphasis of focus, in both industries, falls on improvement when it should, far rather be placed on innovation. We assume, erroneously, that current tools and systems are fit for purpose when history suggests otherwise. When $500 billion doesn’t change the charitable health landscape, we need innovation.
YOU DON’T CHANGE THE SYSTEM, YOU BUILD A NEW ONE THAT MAKES THE OLD ONE OBSOLETE.
BUCKMINSTER FULLER
True innovation does not seek to improve but rather it reinvents, and to do this, its starting point is always a desired outcome to a problem and one driving question. How to best achieve that. Only then, can existing solutions be properly evaluated and their functional worth determined. This process is disruptive in the true sense of the word. It can threaten established financial models, undermine the status quo and realign entire sectors of an industry. For these reasons, in healthcare, a protectionist policy of iteration is favored over innovation.
Better not to rock the boat, even if it is sinking.
Healthcare and the charities providing access to care do not, historically, encourage true innovation, and this, primarily, is why we see diminishing levels of care, prohibitive pricing, dependencies, profiteering and other ills that befall both sectors. Patching a leaky ship has only one eventual outcome.
The desire to repeatedly apply the same patches to the same holes indicates there is more at play in the charity sector than just ill conceived or poorly executed projects.
References
A woman dies of pregnancy related causes every two minutes. What? Globally, maternal mortality rates are…
If your charity or non-profit relies on donations from foundations and the general public, are…
We're thrilled to announce that as of the 17th of July, 2023, our nonprofit Provider…
JULY 02, 2023, AUSTIN, TX – Clinics IV Life, a Texas-based nonprofit led by a global…
MAY 30, 2023, AUSTIN, TX – Clinics IV Life, a Texas-based not-for-profit led by a…
Kung ito ang iyong unang sanggol, malamang na nalantad ka lang sa isang bagong mundo…
{kind=link}